Perthes Disease Treatment
Expert Pediatric Hip Care in Indore
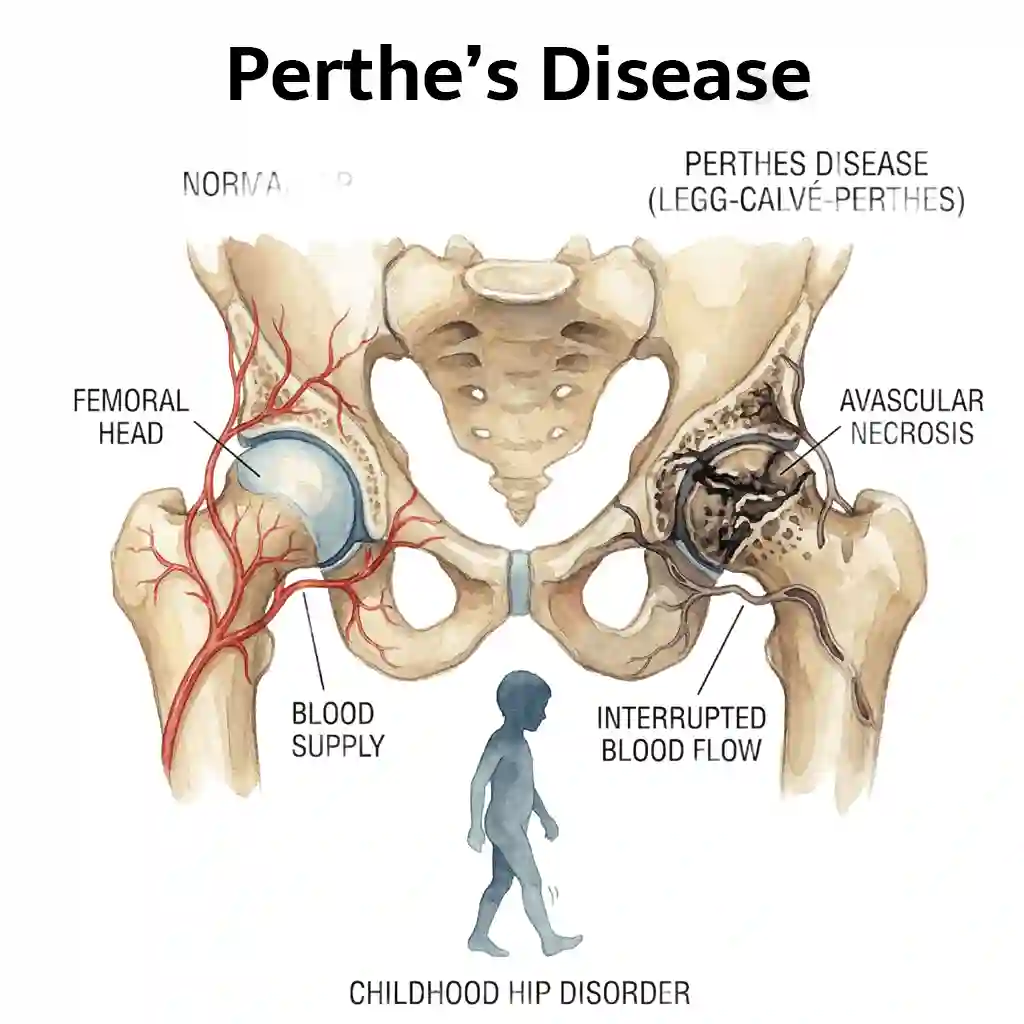
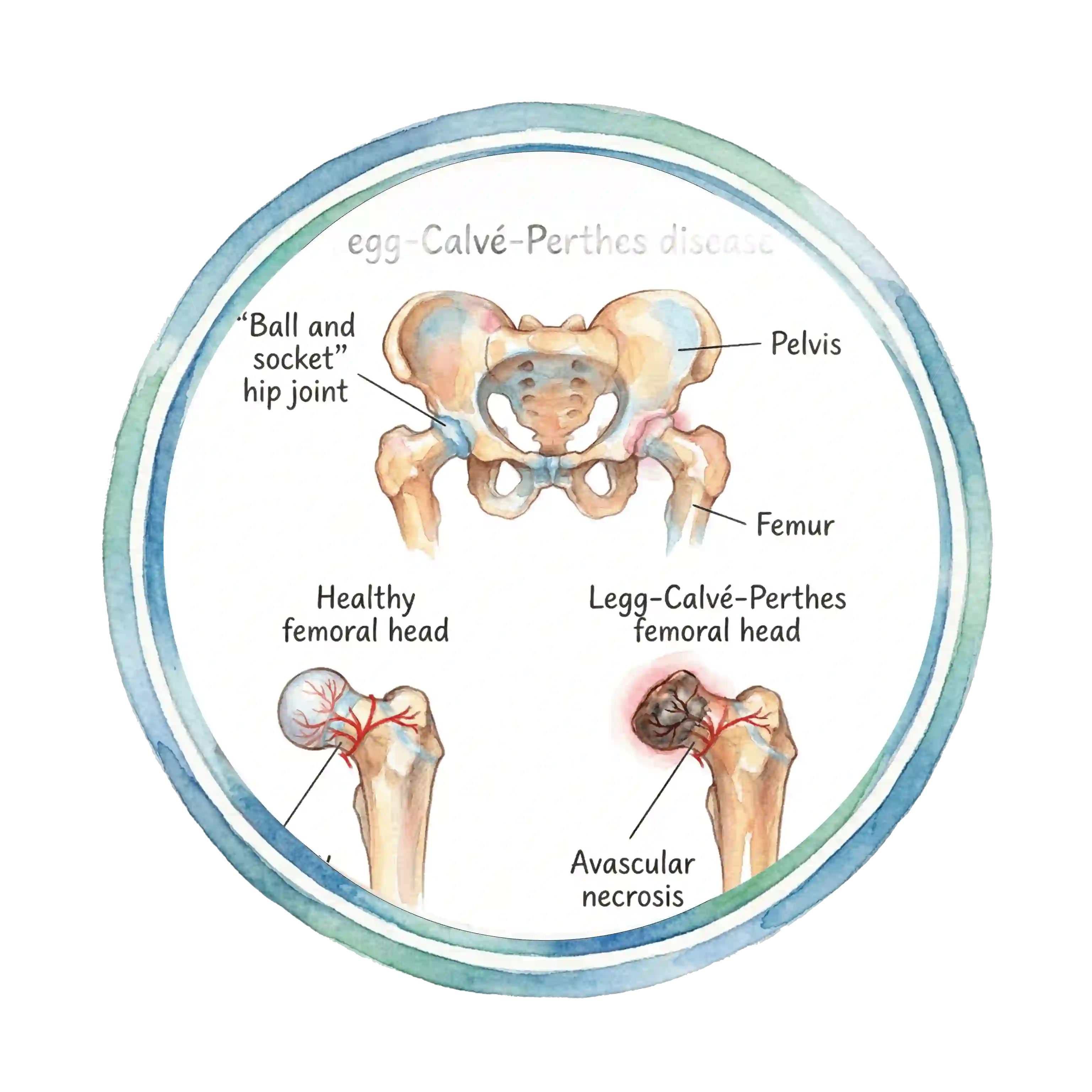
What is Perthes Disease?
Perthes disease, also known as Legg-Calvé-Perthes disease, is a childhood hip disorder that affects the ball (femoral head) of the hip joint. It occurs when blood supply to the femoral head is temporarily interrupted, causing the bone tissue to die (avascular necrosis).
Over time, the blood supply returns and the bone heals. However, without proper treatment, the femoral head may become deformed, leading to hip problems in later life. Early diagnosis and treatment are crucial for the best outcomes.
Who Gets Perthes Disease?
Age Group
Most common in children aged 4-10 years, with peak incidence at 5-7 years
Gender
Boys are 4-5 times more likely to develop Perthes disease than girls
Risk Factors
Family history, secondhand smoke exposure, low birth weight, and certain genetic factors
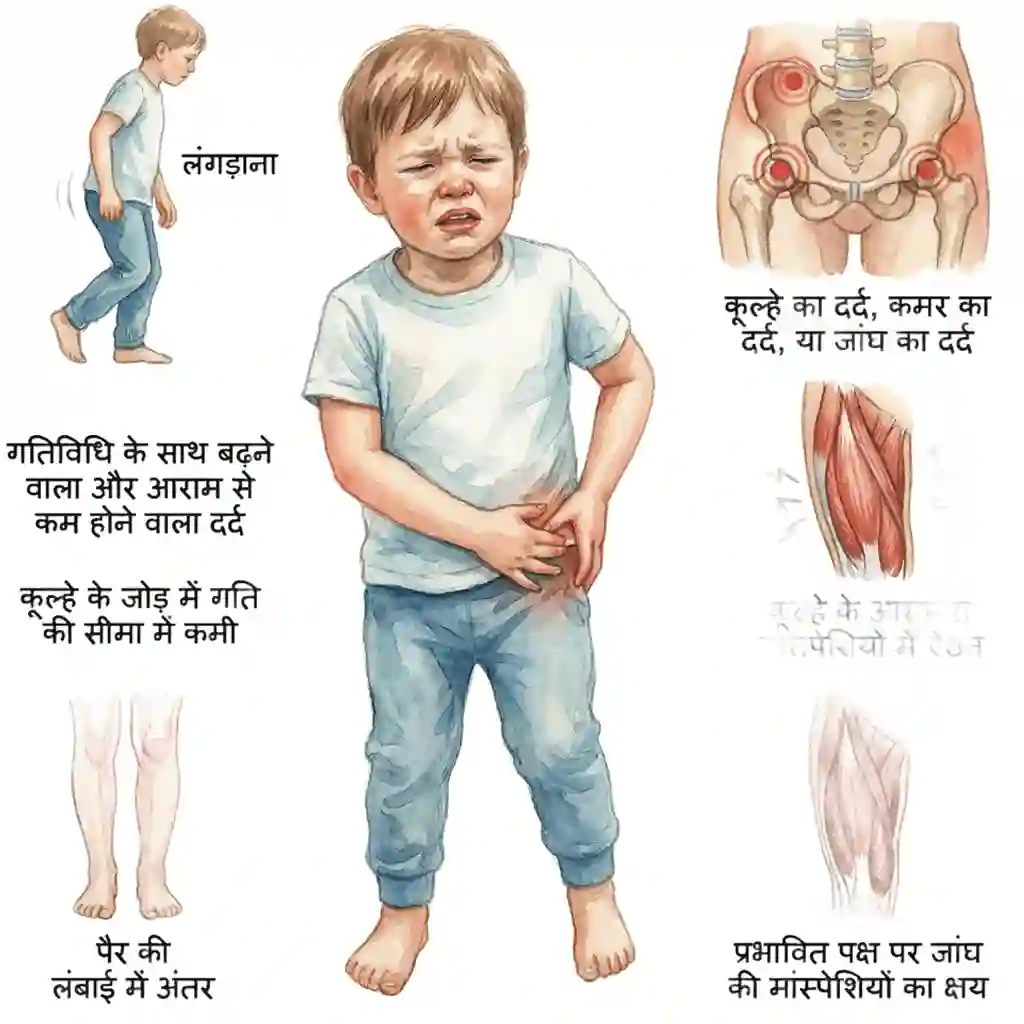
Symptoms and Signs
Early recognition of symptoms is crucial for timely treatment:
- Limping, especially after physical activity or by the end of the day
- Hip pain, groin pain, or thigh pain (sometimes knee pain)
- Reduced range of motion in the hip joint
- Muscle spasms around the hip
- Leg length discrepancy (affected leg may appear shorter)
- Thigh muscle wasting (atrophy) on the affected side
- Pain that worsens with activity and improves with rest
Stages of Perthes Disease
Perthes disease progresses through four distinct stages over 2-4 years:
Initial Stage (Necrosis)
Blood supply is interrupted; bone cells die. Lasts 6-12 months. Child may experience pain and limping.
Fragmentation Stage
Dead bone breaks down and is absorbed by the body. The femoral head may flatten. Lasts 1-2 years.
Re-ossification Stage
New bone forms and strengthens. Blood supply returns. This stage lasts 1-2 years. Treatment focuses on maintaining hip shape.
Healed Stage
Bone healing is complete. The shape of the femoral head determines long-term outcomes. Well-shaped heads have excellent prognosis.
How is Perthes Disease Diagnosed?
X-rays
Primary diagnostic tool showing bone changes, femoral head shape, and disease stage. Multiple X-rays taken over time track disease progression.
MRI Scan
Provides detailed images of bone and soft tissue. Helps detect early changes before they appear on X-rays and assesses blood supply to the femoral head.
Bone Scan
Uses radioactive tracer to evaluate blood flow and bone metabolism. Useful for early diagnosis and determining disease extent.
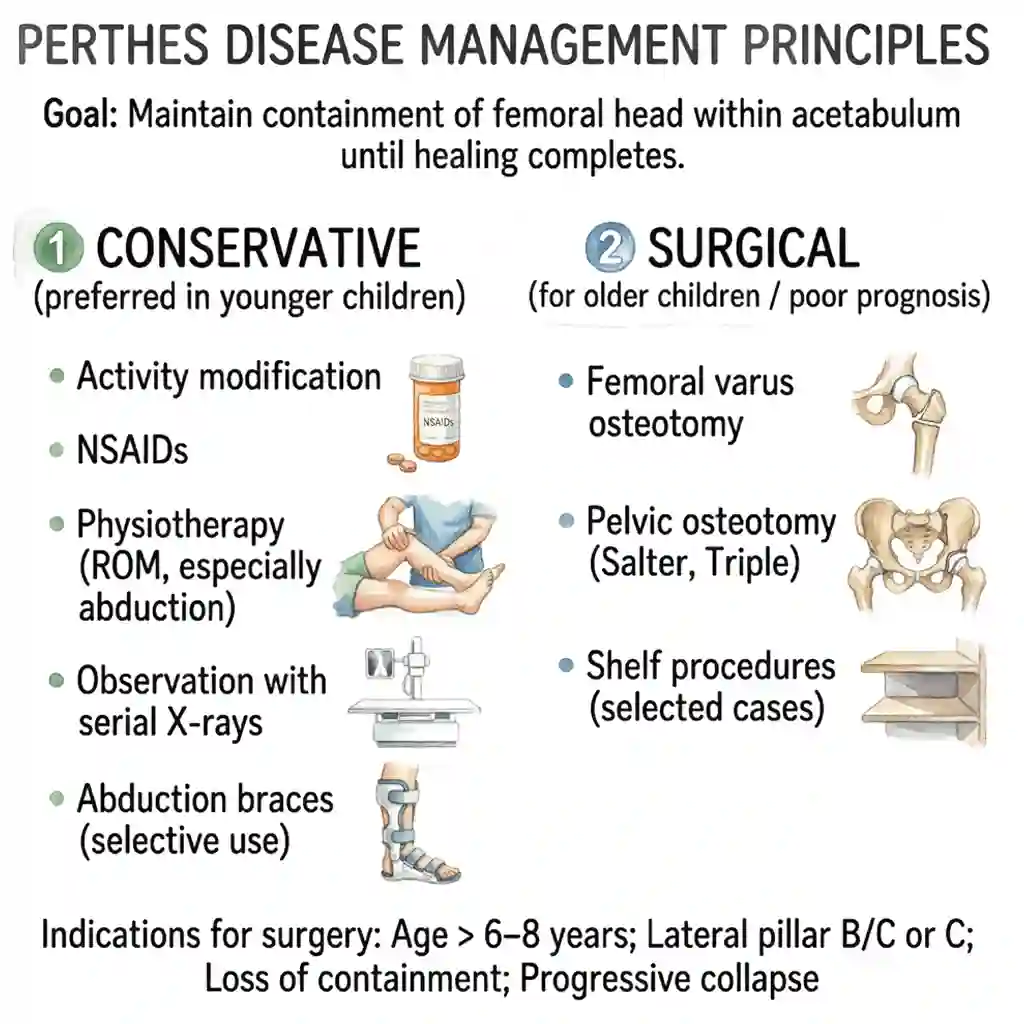
Treatment Options for Perthes Disease
Treatment goals are to reduce pain, maintain hip motion, and keep the femoral head round as it heals. Treatment depends on age, disease stage, and severity:
Non-Surgical Treatment
- Observation and regular monitoring with X-rays (for young children with mild disease)
- Activity modification - avoiding high-impact activities like running and jumping
- Physical therapy to maintain hip range of motion and strengthen surrounding muscles
- Anti-inflammatory medications to reduce pain and inflammation
- Casting or bracing (in selected cases) to keep the femoral head in the hip socket
- Swimming and cycling - low-impact exercises that maintain fitness without stressing the hip
Surgical Treatment Options
Surgery aims to improve hip coverage and containment of the femoral head during the healing process. Various surgical procedures are available, each with specific indications and timing:
VDRO (Varus Derotational Osteotomy)
What is VDRO?
A femoral osteotomy procedure that repositions the femoral head deeper into the acetabulum (hip socket) by cutting the femur and realigning it in a varus (inward) position with derotation.
Indications
- Children older than 6-8 years with poor femoral head containment
- Lateral pillar B or C classification
- More than 50% femoral head involvement
- Hinged abduction on clinical examination
Timing
Best performed during fragmentation or early reossification stage. Should be done when hip still has adequate range of motion.
Benefits
- Improves femoral head coverage
- Reduces hinge abduction and impingement
- Better long-term hip shape and function
Recovery
6-8 weeks non-weight bearing with crutches, followed by gradual weight bearing. Full recovery typically takes 4-6 months. Hardware removal may be needed after 12-18 months.
Shelf Procedure (Chiari Osteotomy)
What is Shelf Procedure?
A pelvic osteotomy that creates a bony shelf over the femoral head to improve lateral coverage. The ilium is cut and displaced medially to create additional coverage for the femoral head.
Indications
- Older children (>8 years) with inadequate lateral coverage
- Severe femoral head deformity or asphericity
- Late presentation in fragmentation or reossification stage
- When femoral osteotomy is not suitable
Timing
Can be performed in fragmentation or reossification stage. Often used as salvage procedure in late-presenting cases or when other surgeries have failed.
Benefits
- Provides lateral support and coverage
- Reduces joint pressure and prevents further deformity
- Can be used even with severe deformity
Recovery
6-8 weeks protected weight bearing, followed by gradual return to activities. Full recovery takes 3-6 months. Long-term outcomes depend on severity of initial deformity.
Salter Innominate Osteotomy
What is Salter Osteotomy?
A pelvic osteotomy that redirects the acetabulum by cutting through the innominate bone above the acetabulum and rotating it forward and downward to improve anterior and lateral coverage.
Indications
- Younger children (4-8 years) with inadequate acetabular coverage
- Good hip range of motion and spherical femoral head
- Early to mid-fragmentation stage
- Lateral pillar B classification
Timing
Best performed early in the disease process during fragmentation stage when femoral head is still relatively spherical. Earlier intervention generally gives better results.
Benefits
- Improves anterior and lateral acetabular coverage
- Maintains hip joint congruency
- Single bone cut with good stability
- Predictable outcomes in appropriate candidates
Recovery
4-6 weeks non-weight bearing, then gradual progression to full weight bearing. Physical therapy for hip range of motion. Full activity typically resumed after 3-4 months.
Triple Pelvic Osteotomy
What is Triple Osteotomy?
An advanced pelvic osteotomy involving three bone cuts (pubis, ischium, and ilium) allowing complete reorientation of the acetabulum for maximum correction of coverage deficiency.
Indications
- Older children and adolescents (>10 years) with severe coverage problems
- Severe acetabular dysplasia requiring major correction
- Late stage disease with healed but deformed femoral head
- When simpler procedures are inadequate
Timing
Usually performed in late reossification or healed stage. Reserved for cases where maximum acetabular reorientation is needed. Often done as salvage procedure.
Benefits
- Maximum degree of acetabular reorientation possible
- Can address severe multidirectional coverage deficiency
- Preserves joint anatomy without entering joint
Recovery
8-12 weeks protected weight bearing due to multiple osteotomies. Intensive physical therapy required. Full recovery may take 6-9 months. More complex than single osteotomy procedures.
Combined Femoral and Pelvic Osteotomy
What is Combined Osteotomy?
Simultaneous or staged femoral (VDRO) and pelvic osteotomy (Salter or shelf) to address severe deformity and coverage problems from both femoral and acetabular sides.
Indications
- Severe Perthes disease with both femoral head deformity and acetabular insufficiency
- Lateral pillar C classification in older children
- Hinged abduction with acetabular dysplasia
- When single procedure would be insufficient
Timing
Can be done simultaneously or staged (femoral first, then pelvic 3-6 months later). Decision depends on surgeon preference, patient age, and severity of deformity.
Benefits
- Addresses both femoral and acetabular pathology
- Maximum improvement in hip biomechanics and coverage
- Better long-term outcomes in severe cases
Recovery
More prolonged recovery than single procedures. 8-12 weeks protected weight bearing. Extensive physical therapy needed. Full recovery 6-12 months. If staged, total treatment extends over 12-18 months.
Other Surgical Procedures
Soft Tissue Release
Release of tight hip adductors and iliopsoas to improve hip range of motion before or after osteotomy. Indicated when severe stiffness limits hip abduction.
Arthroscopic Debridement
Minimally invasive removal of loose bodies, damaged cartilage, or osteophytes causing mechanical symptoms or impingement. Used in late stage for symptomatic relief.
Femoral Head Reduction (Cheilectomy)
Removal of bony overgrowth or prominence from femoral head to reduce impingement. Indicated when femoral head asphericity causes painful mechanical symptoms despite healing.
Hip Arthrodesis (Fusion)
Rarely used salvage procedure fusing hip joint in cases of severe joint destruction with intractable pain unresponsive to other treatments. Reserved for extreme cases only.
Hip Replacement (in Adulthood)
Total hip arthroplasty may eventually be needed in adulthood if severe deformity leads to early arthritis. Modern implants and techniques provide good outcomes even in young adults with Perthes sequelae.
Choosing the Right Surgery
The choice of surgical procedure depends on multiple factors including child's age, disease stage, severity of involvement, femoral head shape, acetabular coverage, and range of motion. Dr. Gaurav Jain will perform thorough evaluation and discuss the most appropriate surgical option for your child's specific condition.
Not all children with Perthes disease require surgery. Many cases, especially in younger children with mild disease, can be successfully managed with observation and non-surgical treatment. Surgery is reserved for cases where maintaining proper hip shape and function requires surgical intervention.
Long-term Outlook
The prognosis for Perthes disease varies based on several factors:
Good Prognosis Factors
- Younger age at diagnosis (under 6 years)
- Less than 50% femoral head involvement
- Lateral pillar A or B classification
- Maintained spherical femoral head shape
Poor Prognosis Factors
- Older age at diagnosis (over 8 years)
- More than 50% femoral head involvement
- Lateral pillar C classification
- Severe femoral head flattening or deformity
With appropriate treatment, most children with Perthes disease can lead active, normal lives. However, some may develop hip arthritis earlier in adulthood, particularly those with poor femoral head shape at healing. Regular follow-up through skeletal maturity and into adulthood is important to monitor hip health.
विशेषज्ञ वीडियो
Expert Videos
डॉ. गौरव जैन द्वारा सेरेब्रल पाल्सी के उपचार और प्रबंधन पर विशेषज्ञ जानकारी
Expert insights on Cerebral Palsy treatment and management by Dr. Gaurav Jain

Frequently Asked Questions
Common questions about Perthes disease answered by Dr. Gaurav Jain
Perthes disease (Legg-Calvé-Perthes disease) is a childhood condition where blood supply to the hip's ball joint is temporarily interrupted, causing bone death and deformity. Over time, blood supply returns and the bone heals, though treatment helps maintain proper hip shape.
Perthes disease typically affects children between 4 and 10 years of age, with peak incidence at 5-7 years. It is more common in boys than girls (4-5 times more likely).
Yes, with proper treatment and monitoring, most children recover well. The bone heals itself over 2-4 years. Treatment focuses on maintaining the round shape of the femoral head during healing to prevent long-term hip problems.
Not all children need surgery. Many children, especially younger ones with mild disease, can be managed with observation and physiotherapy. Surgery is recommended for older children (>8 years), severe cases, or when the hip is at risk of deformity. Dr. Gaurav Jain will evaluate your child and recommend the best treatment approach.
Activity modification is recommended during treatment. High-impact sports like running, jumping, and contact sports should be avoided. However, low-impact activities like swimming and cycling are usually encouraged as they maintain fitness without stressing the hip. Your child can gradually return to sports after healing is complete.
VDRO (Varus Derotational Osteotomy) is a surgery that repositions the femoral head deeper into the hip socket by cutting and realigning the thigh bone. It's recommended for older children (>6-8 years) with poor femoral head coverage, lateral pillar B or C classification, or more than 50% femoral head involvement. The goal is to improve hip coverage and prevent deformity during healing.
The disease typically runs its course over 2-4 years through four stages: necrosis, fragmentation, reossification, and healed stage. Treatment and monitoring continue throughout this period. If surgery is needed, recovery takes an additional 4-6 months for most procedures, though complete bone healing continues over the disease course.
If the hip heals with good spherical shape, the risk of early arthritis is low and most patients do well long-term. However, poor healing with significant deformity may increase the risk of developing arthritis earlier in adulthood. This is why proper treatment to maintain hip shape during healing is so important. Regular follow-up allows monitoring of hip health into adulthood.
In 10-15% of cases, both hips can be affected, though usually not at the same time. If one hip is affected, the other hip should be monitored carefully for signs of the disease. Bilateral Perthes disease (affecting both hips) typically requires more intensive treatment and monitoring.
Femoral osteotomy (like VDRO) cuts and repositions the thigh bone to improve how the femoral head sits in the socket. Pelvic osteotomy (like Salter or shelf procedures) cuts and repositions the pelvis to improve coverage of the femoral head by the acetabulum. Sometimes both procedures are needed together for severe cases. The choice depends on your child's specific anatomy and disease severity.
Expert Care for Your Child
Dr. Gaurav Jain provides comprehensive evaluation and personalized treatment for Perthes disease
Book Appointment: +91-9111464959